
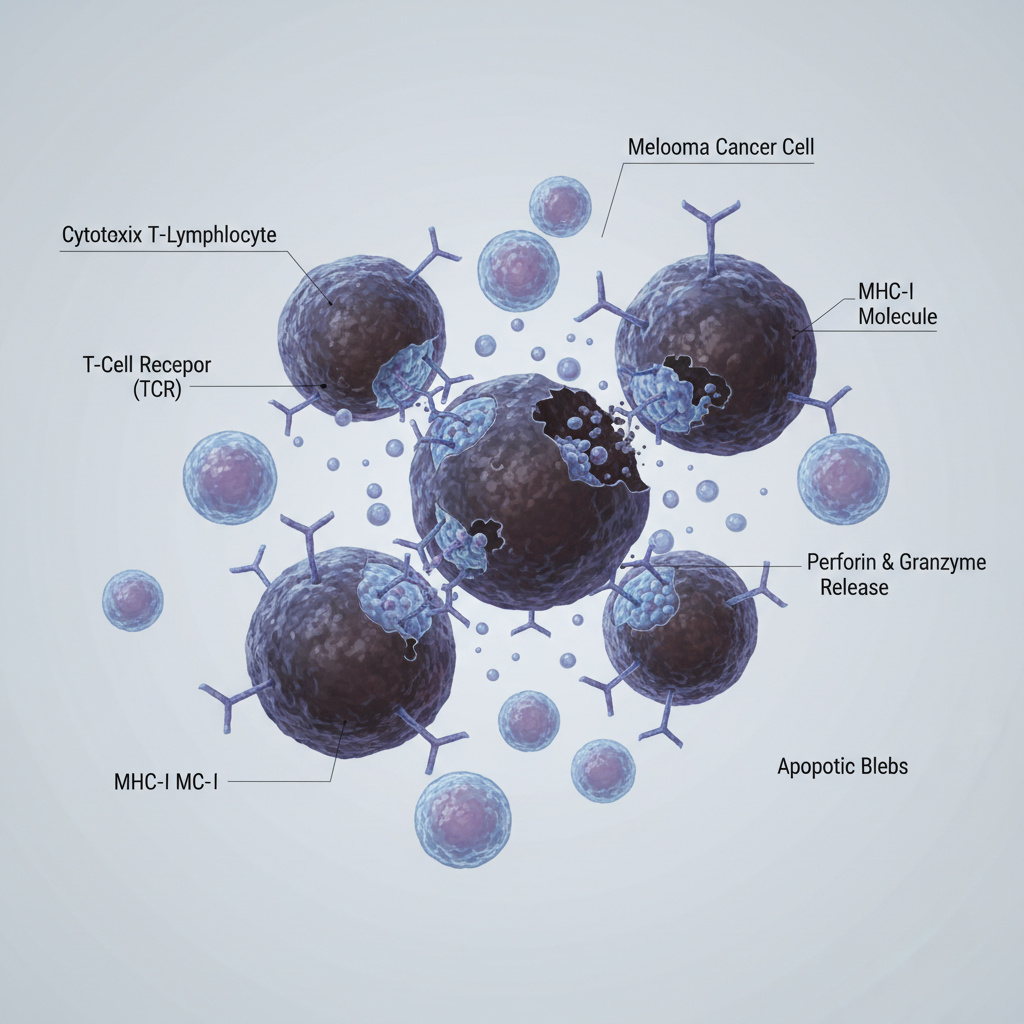
Innovative Therapy for Melanoma
Head and Neck Oncology in Israel — Diagnosis and Treatment at TAMC
Head and neck cancers are never simple. They sit close to vital nerves, vessels, speech and swallowing centers — so every decision has to be precise.
That’s why treatment isn’t about one doctor or one step; it’s about coordination.
At Tel Aviv Medical Clinic (TAMC), we start fast but think carefully.
A patient usually comes in, sees our ENT-oncologist, sometimes the same day we do an endoscopy or a quick ultrasound.
CT or MRI follows, and if we need a biopsy, it’s done under local anesthesia — no waiting weeks for answers.
After that, we all sit down — the ENT surgeon, the oncologist, the radiotherapist, the pathologist.
Everyone brings their piece of the puzzle.
Within a few days, the patient already knows the full picture and the plan — clear, personal, and realistic.
What Conditions Do We Treat?
Lip Cancer
Usually related to prolonged sun exposure or tobacco use.
Treatment focuses on function and appearance preservation — precise surgery with reconstructive options if needed.
In early stages, organ-preserving excision is enough; in advanced cases, plastic reconstruction restores both form and function.
Oral Cavity Cancer
Includes tumors of the mouth floor, cheeks, palate, and inner lips.
Diagnosis starts with clinical exam and biopsy, followed by MRI/CT to determine the spread.
Treatment combines surgery with clear margin control, neck dissection if lymph nodes are at risk, and IMRT/VMAT radiotherapy for high-risk cases.
Speech and swallowing rehabilitation start early to prevent long-term complications.
Thyroid Cancer
Differentiated thyroid cancers (papillary, follicular) often require thyroidectomy with selective lymph node dissection.
Depending on pathology, radioiodine therapy is used afterward to eliminate residual tissue.
For medullary or anaplastic variants, the focus shifts toward targeted therapy or systemic options, combined with radical surgery.
Intraoperative nerve monitoring helps preserve the recurrent laryngeal nerve and reduce voice complications.
Ear Cancer
A rare but challenging group of tumors affecting the ear canal or temporal bone.
Diagnosis requires early biopsy and high-resolution CT.
Treatment includes oncologic resection (up to subtotal temporal bone removal), often followed by radiotherapy.
The main goals: radical tumor control and hearing preservation whenever possible.
Throat and Pharyngeal Cancers
Symptoms often include hoarseness, pain while swallowing, or the feeling of a “lump in the throat.”
Israeli protocols focus on organ-preserving techniques:
- TLM (Transoral Laser Microsurgery) and robot-assisted approaches for early stages;
- combined radiotherapy and systemic therapy for locally advanced disease.
For HPV-associated oropharyngeal tumors, Israel leads in de-escalation protocols — minimizing toxicity while keeping high cure rates.
Salivary Gland Tumors
Includes pleomorphic adenocarcinomas and mucoepidermoid carcinomas.
Treatment balances radical surgery with facial nerve preservation.
Parotidectomy with intraoperative nerve monitoring is standard; if the tumor is aggressive, adjuvant radiotherapy follows.
Reconstruction is performed immediately, during the same operation.
Tongue Cancer
Front-tongue tumors are usually treated surgically, with lymph node assessment.
If pathology shows aggressive features, radiation or chemoradiation may be added.
Speech therapy and oral care begin before radiotherapy to maintain quality of life.
How Treatment Is Performed in Israel
Diagnosis
ENT-oncology consultation with endoscopy, neck CT/MRI, ultrasound, fine-needle aspiration, and full pathology with immunohistochemistry.
When indicated — PET-CT for staging.
Surgery
From organ-preserving resections to extended operations with immediate reconstruction (forehead, radial, or microvascular flaps).
The aim is not just to remove the tumor, but to preserve speech, swallowing, and breathing function.
Radiotherapy
Modern techniques like IMRT and VMAT precisely target the tumor while sparing salivary glands and taste buds.
In certain cases, stereotactic radiosurgery is used for recurrent or limited lesions.
Systemic Therapy
Chemotherapy when indicated, targeted drugs for specific mutations (e.g., RET, NTRK in thyroid cancer), and immunotherapy for selected patients.
Support and Rehabilitation
Dental preparation before radiation, early nutrition support, speech therapy, and oral care are integral parts of the plan.
We manage pain, prevent mucositis, and monitor long-term complications like xerostomia.
Why Patients Choose Israel and TAMC
- Fast scheduling: Full diagnostic workup and treatment planning take days, not weeks.
- Team approach: Every case discussed by head & neck surgeons, oncologists, radiologists, and pathologists.
- Technology: Robotic surgery, intraoperative nerve monitoring, microvascular reconstruction, IMRT/VMAT, and radioiodine therapy when indicated.
- Personalized care: Based on tumor histology, molecular markers, and patient preferences.
For a private consultation with Dr. Inbar Finkel or Dr. Orit Gotfild:
Phone: +972-73-374-6844
Email: [email protected]
WhatsApp: +972-52-337-3108

Prof. Dvora Blumenthal
Neurology
Oncology
Neurologist, neuro-oncologist, head of the neuro-oncology department

Dr. Alexandra Bittan
Oncology
Radiotherapy
Neuro-oncologist and radiosurgery expert

Dr. Amir Sternheim
Onco - Orthopedics
Oncology
Leading Orthopedic Oncologist in Tel Aviv

Dr. Orit Gotfeld
Oncology
Radiotherapy
Radiation Oncologist Specializing in Head & Neck Tumors

Dr. Roman Meirovitz
Oncology
Leading Israeli Oncologist for Lung and Gastrointestinal Cancers

Dr. Stefansky Irena
Oncology
Breast and Gastrointestinal Cancer Specialist

Dr. Daniel Keizman
Oncology
Oncologist and Head of the Urologic Oncology Unit at Ichilov Medical Center

Dr. Yael Bar
Oncology
Medical Oncologist | Breast Cancer Specialist

Dr. Felix Bukshtein
Neurology
Oncology
Senior Neurologist & Neuro-Oncology Specialist

Dr. Inna Ospovat
Oncology
Radiotherapy
Oncologist, radiologist, head of the pediatric radiology department

Dr. Dror Levin
Hematology
Oncology
Pediatric Hematologist–Oncologist | Blood Disorders and Sarcomas in Children

Dr. Postovsky Sergey
Hematology
Onco - Orthopedics
Oncology
Director of Pediatric Hematology-Oncology at Maimonides Medical Center

Prof. Ido Wolf
Oncology
Ведущий онколог Израиля, специалист в области опухолей желудочно-кишечного тракта

Prof. Ofer Merimsky
Oncology
Oncologist, Deputy Director of the Oncology Center, Head of Bone and Soft Tissue Oncology Unit

Prof. Ravit Geva
Oncology
Medical Oncologist | Gastrointestinal Cancer Specialist

Dr. Tatiana Rabin
Oncology
Radiotherapy
Senior Oncology Specialist, Director of the Gynecological Oncology and Brachytherapy Service of the Oncology Department

Dr. David Sarid
Oncology
Oncologist, head of oncological urology, oncology system

Prof. Tamar Safra
Oncology
Gynecologist, oncologist, head of the gynecological oncology service at the oncology department
What diseases does Head & Neck cancer Clinic treat?
- Lip Cancer
- Oral Cancer
- Thyroid Cancer
- Ear Cancer
- Throat Cancer
- Salivary Gland Cancer
- Tongue Cancer
FAQ: Dr. Inbar Finkel — Oncologist, Head of the Head & Neck Oncology
How is radiotherapy combined with other treatments in head and neck cancer?
It’s rarely used alone. In most cases, radiotherapy works best together with surgery or chemotherapy.
The goal isn’t just to destroy tumor cells — it’s to protect what matters: speech, swallowing, and taste.
We plan radiation fields with millimeter precision, using IMRT or VMAT, so that healthy tissues stay functional.
It’s a delicate balance, and every plan is built around the person, not the diagnosis.
Can all head and neck tumors be treated while preserving function?
Not always, but we try whenever possible.
Our main principle is preserve, if safe.
I’ve seen patients return to normal speech and eating just weeks after surgery and radiation.
That’s why early diagnosis is everything — the earlier we act, the more we can save.
What’s special about the way TAMC manages complex head and neck cancers?
Coordination. Everything happens fast, but nothing is rushed.
ENT surgeons, radiation oncologists, and medical oncologists sit together, discuss scans, pathology, and options — in one room.
That’s how we avoid delays and give patients a clear, confident plan within days.
FAQ: Dr. Orit Gotfild — Director, Institute of Radiotherapy
What does modern radiotherapy look like for head and neck cancers?
Very different from what people imagine.
It’s not about “burning” the tumor anymore — it’s about sculpting the dose.
With IMRT and VMAT, we shape the radiation beam around critical structures like salivary glands or vocal cords.
Patients keep their ability to speak and taste. That’s the progress of the last decade.
When is radioiodine therapy used for thyroid cancer?
Only when it’s truly needed. Radioiodine is very effective for differentiated thyroid cancers, but it’s not for everyone.
We base that decision on pathology and molecular markers — if there’s microscopic disease left or lymph node involvement, then yes, we do it.
The idea is to treat enough, but not more than necessary.
Is radiotherapy in Israel painful or difficult to go through?
It’s not painful, but it can be tiring. The sessions are short — about 10–15 minutes each — and patients come daily for several weeks.
We support them through nutrition, pain management, and oral care.
Most people continue to live their normal lives during treatment, just a bit slower, and that’s okay.


Contact form























