
 Contact Us
Contact Us Innovative Therapy for Melanoma
What is this?
What is immunotherapy
Immunotherapy is one of the modern approaches used in oncology, where the patient’s own immune system is involved in the process.
In practical terms, the goal is not always to destroy the tumor directly, but to help the immune system recognize it and start reacting.
In real clinical situations, the issue is usually not that the immune system “doesn’t work.”
More often, it simply does not identify the tumor as a threat.
How it works?
How immunotherapy works
Under normal conditions, the immune system constantly monitors the body.
It is capable of detecting infections, and in some cases — abnormal or tumor cells.
However, a tumor is not a foreign agent like a virus.
It develops from the body’s own cells and can effectively “hide” from immune surveillance.
As a result:
- the immune system may not detect it
- or detects it but does not respond
- or the response is insufficient
Immunotherapy works through different mechanisms. Some treatments help the immune system recognize tumor cells again, while others enhance an existing immune response or direct it toward specific targets.
In clinical practice, this distinction matters, because different tumors escape immune control in different ways. Treatment is therefore selected based not on the name of the method, but on the biology of the specific tumor.
When is it used?
When immunotherapy is used
Immunotherapy in Israel is rarely used as a standalone treatment.
In most cases, it is considered:
- as part of combination therapy
- in advanced stages of disease
- in recurrent disease
- when standard treatment options are no longer effective
In certain situations, immunotherapy may be considered as a first-line treatment. However, this is not a universal approach.
The decision depends on the tumor type, its molecular characteristics, and how the disease behaves in a specific case. In practice, this is always an individual decision — there is no single scenario that applies to all patients.
Types
Types of immunotherapy
Immunotherapy is not a single treatment, but a group of different approaches.
- Checkpoint inhibitors
The most widely used group. These drugs block mechanisms that tumors use to suppress the immune response.
Examples include:
- PD-1
- PD-L1
- CTLA-4
The introduction of these therapies significantly changed clinical practice in oncology and expanded treatment options in a number of diseases, especially where previous options were limited.
- Monoclonal antibodies
These drugs target specific molecules on the surface of tumor cells.
Depending on the mechanism, they may:
- block tumor growth
- “mark” cancer cells for the immune system
- enhance the effect of other treatments
- Cell-based therapies (including CAR-T)
One of the most complex and advanced approaches.
The concept involves:
- collecting immune cells from the patient
- modifying them in a laboratory setting
- returning them back to the body
After reinfusion, these cells are able to recognize and respond to tumor cells.
This approach is not used in all cancers. It is most commonly applied in hemato-oncology, where there is already substantial clinical experience and established outcomes.
- Cancer vaccines
Cancer vaccines represent a separate direction within immunotherapy.
Some of these approaches are still under investigation, while others are already used in clinical practice. One example is Sipuleucel-T, used in prostate cancer.
The goal is not direct tumor destruction, but activation of the patient’s immune system to recognize tumor-related antigens.
- Immune response modulators
These drugs affect the immune system more broadly rather than targeting a specific tumor.
Examples include interferons and interleukins.
They were used more frequently in the past, but their role has declined due to side effects and the emergence of more targeted therapies. In selected cases, however, they may still be considered.
What diseases is it used for?
In which cancers immunotherapy is used
Immunotherapy is now considered as part of treatment in a range of oncological diseases.
However, its role varies depending on tumor type, molecular profile, and disease stage.
- Non-small cell lung cancer
One of the key areas where immunotherapy has become standard.
Commonly used drugs include:
- Pembrolizumab (Keytruda)
- Nivolumab (Opdivo)
- Atezolizumab (Tecentriq)
These may be used alone or in combination with chemotherapy.
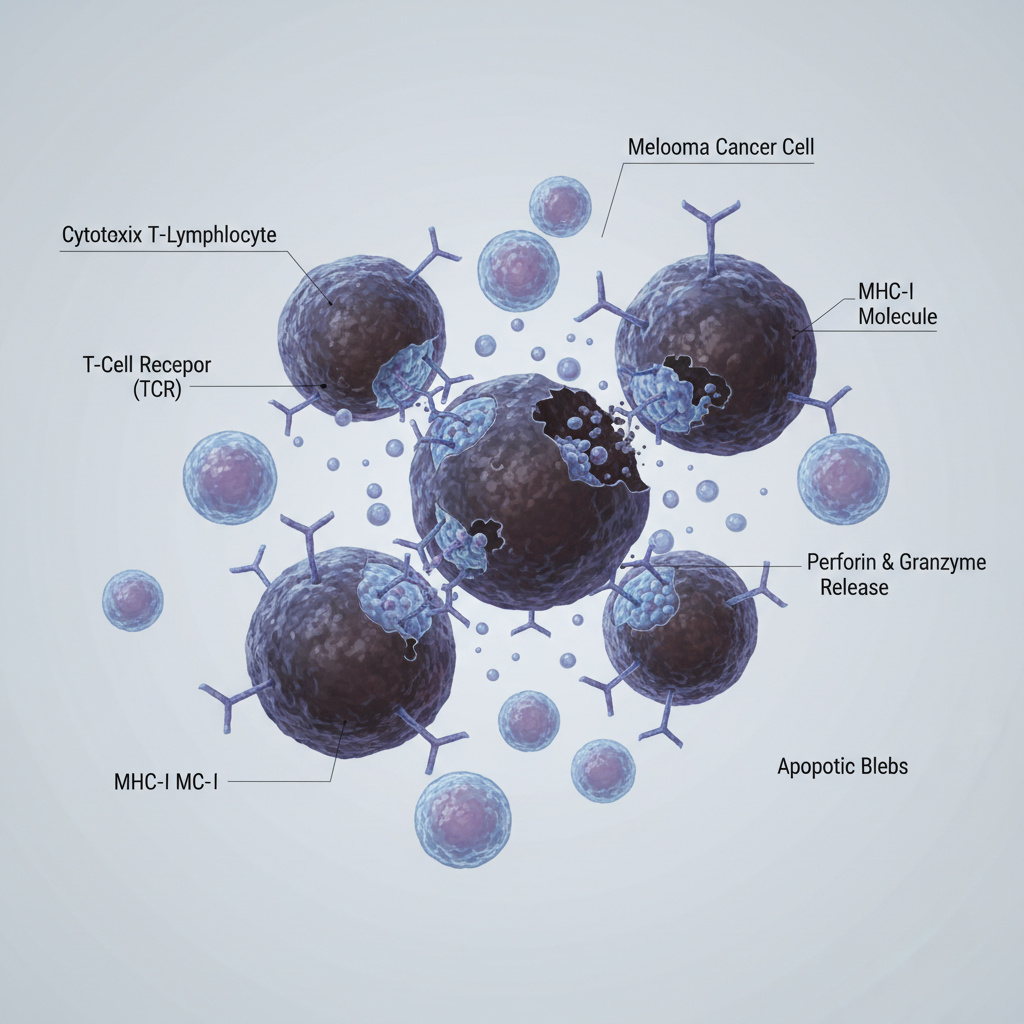
- Melanoma
One of the first cancers where immunotherapy demonstrated a significant clinical impact.
Used treatments:
- Nivolumab (Opdivo)
- Pembrolizumab (Keytruda)
- Ipilimumab (Yervoy)
Combination therapy (nivolumab + ipilimumab) is used in advanced stages.
- Kidney cancer
Immunotherapy is often combined with targeted therapy.
Examples:
- Nivolumab + Ipilimumab
- Pembrolizumab + Axitinib
- Bladder cancer
Used in advanced disease or after progression following chemotherapy.
- Pembrolizumab
- Atezolizumab
- Nivolumab
- Breast cancer (triple-negative)
Used in selected cases with specific biomarkers (e.g., PD-L1).
– Pembrolizumab (in combination with chemotherapy)
- Gastric and esophageal cancer
Used in advanced disease.
- Nivolumab
- Pembrolizumab
- Liver cancer (hepatocellular carcinoma)
Recent combinations include:
- Atezolizumab + Bevacizumab
- Durvalumab
- Cervical cancer
Used in recurrent or metastatic disease.
– Pembrolizumab
- Lymphomas (B-cell)
Includes both antibody-based and cellular approaches:
- Rituximab
- CAR-T therapies (Kymriah, Tecartus)
- Acute lymphoblastic leukemia (B-ALL)
Used in relapsed or refractory disease:
- CAR-T therapy
- Blinatumomab
- Multiple myeloma
Emerging CAR-T approaches:
- Idecabtagene vicleucel
- Ciltacabtagene autoleucel
- Prostate cancer
Limited use, but includes:
– Sipuleucel-T (Provenge)
- Head and neck cancers
Used in advanced disease:
- Pembrolizumab
- Nivolumab
👉 More details about specific drugs and treatment approaches are available in the dedicated section: Immunotherapy: main drug groups
What is important to understand
Despite its broad use, immunotherapy is not suitable for every patient.
The decision depends on:
- tumor type
- molecular markers
- stage of disease
- previous treatments
Treatment is always individualized.
Side effects
Side effects
The side effect profile of immunotherapy differs from chemotherapy and is related to its mechanism of action.
Rather than directly damaging rapidly dividing cells, immunotherapy activates the immune system, which may lead to an excessive immune response.
Possible effects include:
- fatigue
- low-grade fever
- skin reactions
- inflammatory changes in different organs
In some cases, immune-related adverse events may occur, affecting:
- lungs (pneumonitis)
- intestines (colitis)
- liver (hepatitis)
- endocrine system (thyroid or adrenal dysfunction)
Most side effects can be managed if identified early, which is why regular monitoring is essential.
Treatment decision
How treatment decisions are made
The decision to include immunotherapy in a treatment plan is made individually.
It is based on a comprehensive evaluation of:
- tumor type and stage
- molecular characteristics (including PD-L1 expression)
- overall condition
- previous treatments
In some cases, multiple treatment options exist, including combination approaches. The final choice depends on expected benefit, safety profile, and clinical context.
Immunotherapy and clinical trials
In certain clinical situations, participation in a clinical trial may be considered as an additional option, particularly when standard treatments are limited.
However, eligibility depends on strict criteria related to tumor type, stage, previous therapy, and overall condition. Therefore, this option is evaluated individually.
Oncology consultation
Oncology consultation in Israel
If immunotherapy is being considered, or if there are questions regarding treatment, it is reasonable to start with a consultation.
During the consultation:
- medical records are reviewed
- the current clinical situation is assessed
- possible treatment options are discussed
📞 Phone: +972-73-374-6844
📧 Email: [email protected]
💬 WhatsApp: +972-52-337-3108
Important information
The information provided on this page is intended for general informational purposes only and does not constitute medical advice, diagnosis, or a substitute for a personal consultation with a qualified physician.
Tel Aviv Medical Clinic is not a pharmacy and does not supply or dispense medications. Information about drug-based treatments, including chemotherapy and immunotherapy, is presented for general understanding only.
All treatment decisions should be made by the treating physician, based on the patient’s individual medical condition.
If you have any medical questions or need guidance regarding treatment options, please consult your physician.
The medical team

Prof. Dvora Blumenthal
Neurology
Oncology
Neurologist, neuro-oncologist, head of the neuro-oncology department

Dr. Alexandra Bittan
Oncology
Radiotherapy
Neuro-oncologist and radiosurgery expert

Dr. Amir Sternheim
Onco - Orthopedics
Oncology
Leading Orthopedic Oncologist in Tel Aviv

Dr. Orit Gotfeld
Oncology
Radiotherapy
Radiation Oncologist Specializing in Head & Neck Tumors

Dr. Roman Meirovitz
Oncology
Leading Israeli Oncologist for Lung and Gastrointestinal Cancers

Dr. Stefansky Irena
Oncology
Breast and Gastrointestinal Cancer Specialist

Dr. Yair Gortzak
Onco - Orthopedics
Oncology
Head of the National Orthopedic Oncology Department, Ichilov Medical Center, Tel Aviv

Dr. Daniel Keizman
Oncology
Oncologist and Head of the Urologic Oncology Unit at Ichilov Medical Center

Dr. Inbar Finkel
Oncology
Oncologist, Director of the Head and Neck Tumor Department

Dr. Mor Miodovnik
Dermatology
Oncology
Дерматолог и венеролог, врач-онколог

Dr. Sharon Peles
Oncology

Prof. Ido Didi Fabian
Oncology
Ophthalmology
Ocular Oncology Specialist

Dr. Felix Bukshtein
Neurology
Oncology
Senior Neurologist & Neuro-Oncology Specialist

Dr. Inna Ospovat
Oncology
Radiotherapy
Oncologist, radiologist, head of the pediatric radiology department

Dr. Dror Levin
Hematology
Oncology
Pediatric Hematologist–Oncologist | Blood Disorders and Sarcomas in Children

Prof. Baruch Brenner
Oncology
Gastrointestinal Oncology Specialist

Prof. Ido Wolf
Oncology
Ведущий онколог Израиля, специалист в области опухолей желудочно-кишечного тракта

Prof. Ofer Merimsky
Onco - Orthopedics
Oncology
Oncologist, Deputy Director of the Oncology Center, Head of Bone and Soft Tissue Oncology Unit

Prof. Ravit Geva
Oncology
Medical Oncologist | Gastrointestinal Cancer Specialist

Dr. Tatiana Rabin
Oncology
Radiotherapy
Senior Oncology Specialist, Director of the Gynecological Oncology and Brachytherapy Service of the Oncology Department
Frequently Asked Questions
Frequently Asked Questions – Answered by Dr. Stefansky Irena
1. If I have already undergone chemotherapy and it did not help — is there still a point in considering immunotherapy?
This is a question I hear quite a bit.
In some cases — yes. There are situations in which, precisely after the failure of a previous treatment, immunotherapy can be a relevant option. But it depends very much on the type of tumor and its characteristics. Not every case is suitable, so it is important to check it precisely.
2. How long does it take to understand whether the treatment is effective?
There is no one answer that fits everyone.
Sometimes you see a change after a few weeks, and sometimes it takes longer. There are also cases where at first it seems that there is no response — and only later there is improvement. That is why we do not look at just one test, but at the trend over time.
3. Can immunotherapy replace chemotherapy?
In some cases — yes, but not always.
There are situations in which immunotherapy can be used as the main treatment, and there are situations in which it is combined with other treatments. The decision depends on the tumor itself and not just on the preference for one treatment over another.
4. What happens if immunotherapy doesn’t work?
This is a very important point.
If there is no response to treatment, it is possible to move on to other approaches — for example, combination therapies, targeted therapies, or sometimes even clinical trials. It is important to understand that not responding to one treatment does not mean that there are no other options.
5. Is there an advantage to additional counseling before starting treatment?
In my opinion — yes, especially in complex situations.
Sometimes another look at the data can change the direction of thinking or open up options that were not previously considered. This is especially true when it comes to advanced treatments like immunotherapy.


Contact form

Oncology

Hematology

Cardiac surgery

Cardiology

Dermatology

Gastroenterology

Female breast surgery

Endocrinology

Head and neck surgery

Gynecology

Neurology

Nephrology and dialysis

Immunology

Ophthalmology
Oncology

Plastic surgery

Orthopedics

Orthopedic-Oncology

Radiation therapy

Pulmonology

Psychiatry

Urology

Rheumatology


Pediatric Department